

San Diego area doctors seldom complain to their patients about low Medicare pay. But for two long decades, many have complained bitterly to each other.
That's because an old and complex federal formula reimburses physicians here as if they were practicing in "rural" areas, and assumes their costs of rent and staff are low, resembling those in Fresno or El Centro rather than Anaheim or Los Angeles.
"The joke among doctors has been, 'Look at all our cows,'" quipped Dr. James Hay, a family practitioner in Encinitas and former California Medical Association president.
Doctors regard these underpayments, alleged to be in the billions nationally, as a federal snub, with consequences to patient care. The lower rate has depressed the physician supply here, making access to care for Medicare patients tougher. In subtle ways, it has dissuaded some area physicians from accepting Medicare beneficiaries or expanding the number they see, they say.
It also has encouraged "concierge" cash-only practices and lengthened wait times beneficiaries must endure for an appointment.
Now, after a tempestuous 14-year fight and a $5 billion lawsuit that got as far as the U.S. Supreme Court, a congressionally approved fix will gradually increase doctors pay in San Diego County and 14 other California counties that were inappropriately classified. Starting Jan. 1, the new rule, embedded in the Protecting Access to Medicare Act of 2014, will pay them higher rates, more like doctors practicing in Orange County and other higher cost urban areas of the state.
Counties Affected By Medicare Payment Change
Doctors in these California counties will get higher Medicare reimbursement beginning Jan. 1.
El Dorado
Marin*
Monterey
Placer
Riverside
Sacramento
San Benito
San Bernardino
San Diego
San Joaquin
San Luis Obispo
Santa Barbara
Santa Cruz
Sonoma
Yolo
*Marin County will move out of a locality it shares with Solano and Napa counties into its own region, resulting in more pay for Marin physicians.
Other categories of health providers who bill Medicare, such as nurse practitioners, podiatrists and optometrists, may expect more money too.
"We'll be able to have reimbursement that more closely approximates the cost of providing care instead of underpaying us as if we were El Centro," said Dr. Ted Mazer, a San Diego ear, nose and throat specialist who has been among the leaders in the fight to change Medicare's payment formula.
"And, because Medicare rates are followed by virtually all commercial payers here," rates from private insurance companies should rise, too, Mazer said.
Higher payments "will help the viability of our practices, both in attracting new doctors as our older doctors age out, and our existing population grows older and needs more care," he said. And, "it will put money on the table for people to buy new technologies (like electronic health record capabilities)."
Nicknamed "the GPCI fix," the correction changes the geographic practice cost index formula Medicare uses to reflect regional physicians' costs, such as hiring office staff, paying rent and buying malpractice insurance in Medicare's 89 GPCI localities around the country.
Pinpointing a particular event that pushed Congress to make the change is difficult. In the end, Mazer said, it came down to “just good old politics of facts and timing,’’ the support of key elected officials on both sides of the aisle, and the physicians’ persistence.
Elizabeth McNeil, the California Medical Association's vice president for federal government relations, estimated the GPCI fix will bring about $52 million a year more to California providers in these 15 counties that submit Part B Medicare claims, depending on inflation. San Diego County doctors who bill Medicare will get about half of that total.
The GPCI fix still won't bring San Diego County's pay up to Orange County's level, but it's a start.
"That would have been nice," Mazer said, "but that's not what was approved."
About 7,000 San Diego County doctors will be affected, with increases of about 6 percent in increments over the next six years.
Former San Diego County Medical Society CEO Tom Gehring said the change ultimately will add $10,000 to the average doctor's annual payments in this county.
Technically, the new rule requires Medicare to move 15 counties from "locality 99, rest of state," or rural, to regions that use metropolitan statistical area costs to calculate payment. Los Angeles, San Francisco, Orange, Alameda, Solano, San Mateo, Ventura and Santa Clara counties have long had their own metropolitan formula, all of which pay more than locality 99, which covers all of the other California counties.
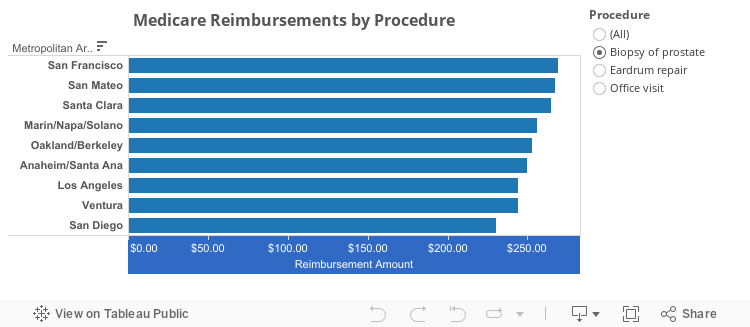
The pay differences are significant. Today Medicare reimburses doctors in the so-called rural counties like San Diego $76.48 for a simple office visit for an established patient, while a few miles north, "urban" Orange County doctors receive $82.19. For procedures, the differences are greater. San Diego gastroenterologists receive $548.57 for a colonoscopy with polyp removal, while in Orange County, the pay is $602.12. San Francisco and Los Angeles rates are even higher.
In fact, the eight currently "urban" areas of the state all have higher reimbursement than San Diego County. For example, cystoscopy and treatment in transurethral surgery pays doctors in those eight areas on average 12 percent, or $34.95, more than it pays doctors in locality 99. A dilation of the esophagus pays 14 percent more.
The adjustment will come in increments; each year San Diego doctors will get one-sixth of the difference between the locality 99 rate and their new MSA rate until the full amount is reached in 2022.
Despite the area's scenic beauty and weather as enticements, doctors here have long complained of the challenge in bringing new doctors to their practices. Interested partners think they'll be paid based on high Southern California costs of living, and they're surprised.
"It's been very hard to recruit in San Diego," said Dr. John LaFata, an internal medicine doctor whose six-physician Vista practice struggled to hire three internists in the last two years.
"I know hospitals have a hard time recruiting cardiologists, general and vascular surgeons and other surgical subspecialists because the cost of living is much higher here. People say, 'I can do much better in Iowa if I can tolerate the weather.' Much of that is due to (Medicare's) differential payment structure."
Dr. Vimal Nanavati, an Otay Lakes critical care cardiologist, said the pay increase will have “a huge impact” on physician practices. It will mean “shorter wait times for patients,” and doctors can spend more time with patients during appointments. “If you’re getting paid less, you have to see more patients. Now, we can take more patients and take our time seeing them. Our practices will be easier to manage.”
Dr. Sherry Franklin, a pediatric endocrinologist in Solana Beach who has some Medicare patients in her solo practice, called the GPCI fix "a win-win for physicians and consumers. Physicians have earned the right to a raise. This will increase access for patients."
Franklin said that over time, the pay increase will allow physicians to "expand the pool of Medicare patients they can afford to see."
Additionally, for commercial plans such as Aetna that follow Medicare reimbursement, more money may translate to better contracts that increase the number of physicians in those plans' networks.
Of course, when physician fees go up in Medicare, so will beneficiaries' 20 percent co-pays under Part B. If Medicare increases a $100 payment to $106, for example, the beneficiary's co-pay goes from $20 to $21.20.
LaFata doesn't think patients will notice, or if they do that they will mind. He said many have supplemental Medicare plans that cover those co-payments. And those who don't will gladly pay the extra money. "Many patients tell me they think we're underpaid anyway."
How did San Diego get labeled rural?
In the 1960s, the Centers for Medicare & Medicaid Services established physician payment rules based on cost of practice formulas in 210 payment localities, adjusting for high cost areas such as New York City and Los Angeles. Back then, San Diego County was a much cheaper place to live and work.
But times changed; San Diego grew as did its costs. Yet when CMS updated GPCI regions in 1996, consolidating payment areas nationally from 210 to 89, it failed to reflect those shifts.
'"And nobody was paying attention," said Dr. Larry de Ghetaldi, an emergency room physician in "rural" Santa Cruz.
Except that de Ghetaldi was paying attention. In 2001, in his dual role as administrator of a surgical center and director of a medical group, he was surprised to see Medicare's wage and cost index paid Santa Cruz hospitals a lot more than the index it used to pay Santa Cruz doctors.
De Ghetaldi and others took their beef to Tom Scully, then CMS administrator. "Why do you use a different set of maps to pay physicians than you do to pay hospitals?" de Ghetaldi asked.
"The answer was, ‘We will look at it.’ And the answer always was, ‘We will look at it,'" he said.
Just up the road, doctors in adjacent Santa Clara County with similar costs and demographics receive pay that is 20 percent higher.
GPCI kings and queens
De Ghetaldi, Mazer, McNeil, Santa Barbara gastroenterologist Edward Bentley, and Rochelle Dornatt, chief of staff for California Congressman Sam Farr, D-Carmel, became obsessed with the issue. They called themselves "the GPCI kings and queens," de Ghetaldi said.
They made dozens of trips to Washington to plead with Medicare officials and lawmakers, but were frequently left waiting for appointments that were canceled or delayed. It was a frustrating time.
In 2007, de Ghetaldi's brother Dario, a Millbrae attorney, filed a $3.2 billion lawsuit against the secretary of the U.S. Department of Health and Human Services on behalf of Mazer and seven "rural" California counties, including San Diego. It was later amended to $5 billion, and was appealed all the way to the Supreme Court.
One such trip was particularly exasperating, Mazer recalled. They were scheduled for a two-day meeting in Medicare's Baltimore headquarters. "It was like going to a military compound. They had mirrors to look under our car."
By mid-morning the group sensed "about as big of a stonewall as you could get," Mazer said. "No matter what we said, they couldn't possibly do it. We were simply asking that they shift physician pay to the system they used for hospitals ... so they wouldn't have two conflicting systems.
Solution after solution was offered, Mazer said, but "CMS just spit in our face and said, 'No, no.'"
The lawsuit seemed like the only way. It sought class-action status for 250 counties across the country that were in the same undervalued boat.
"It questioned several administrators in several presidential administrations, and said publicly, you (CMS) guys knew what you were doing was wrong," Mazer said. "You knew how to fix it. But you just didn't want to fix it. Year after year, the problem kept compounding. And they hurt people in the process."
Ultimately, the Supreme Court refused to recognize the plaintiffs' class action standing and the lawsuit died. But the ”GPCI kings and queens” did not give up.
In Baltimore, Medicare officials argued repeatedly that legally, they could only fix a state's GPCI disparities if each state's own doctors unanimously agreed to a statewide solution.
That's because the physician fee schedule has generally been a zero-sum game; one doctor's pay raise requires another's pay cut. So state medical societies would have to find their own rob-Peter-to-pay-Paul solution. And their decisions would have to be unanimous.
Physician groups dispute that is the law. But they tried that solution too.
A near fistfight on the House floor
"I have four feet of shelf space full of nothing but GPCI files," said Dornatt, whose boss a decade ago introduced a bill that would resolve the problem just within California.
After months of work, Farr, a Central Coast Democrat, had "lined up players on both sides," she said.
"Congressman Bill Thomas, (a Republican representing the Central Valley) who chaired the Ways and Means Committee, his staff was telling me, yes, we'll put it in. Just have Mr. Farr go to the floor and Mr. Thomas will sign off on it.
"But when Mr. Farr went to the floor, Mr. Thomas refused to sign off on it and they almost had a fistfight," Dornatt said. Added Adam Russell, Farr's press representative, Farr "made a fist at Thomas he was so angry."
Thomas reneged in fear that physicians in his rural Central Valley district would be hurt by a new formula that took San Diego and other wealthier counties out of locality 99.
Similar urban/rural cost disparities exist in about 250 counties in other states, including Ohio, Georgia, Maryland and Texas. But efforts to make corrections in those states flamed out. Why? Because in California, there was data; the underpayments couldn't be ignored. Less so elsewhere, Gehring said.
"We made the most noise about it," Dr. Larry de Ghetaldi said.
Over the years, high level reports recognized and addressed the problem. The Urban Institute in 2004, the Government Accountability Office in 2005 and in 2007, the Centers for Medicare & Medicaid Services in 2008, the Institute of Medicine in 2011 and 2012, and the Medicare Payment Advisory Commission in 2013.
Who pays for the GPCI fix?
The GPCI fix law directs CMS to adjust certain overvalued procedures to more accurately reflect the actual work required for that service.
"That means a payment cut" affecting some physicians for some services across the country, McNeil said. Fine details will come with the Physician Fee Schedule rules for 2017 this summer.
The new law also protects rural counties that will remain in locality 99 from having their payments reduced when San Diego and the 14 other counties are reassigned next year.
While he's grateful the fight is finally over, the GPCI fix will not return what doctors lost since 1996, Mazer lamented. And, he's "still ticked off" the correction requires eight years to fully implement.
"There's still a part of me that says, 'you guys ripped us off for years. You should give us something for that.' But it's done. We are where we are."
Ironically, he said, most doctors in counties like San Diego are unaware they'll see more money from Medicare. "It's taken so long to get here, and so long to implement. At least we're moving forward now, and CMS is now ready to do the right thing."




