
If patients want to know rates of potentially deadly hospital-acquired infections at UCSD Medical Center in Hillcrest versus UCSD's Thornton Hospital in La Jolla, they've been out of luck.
That's because Medicare's publicly reported data combines those two hospitals' infection rates, even though their rates of complications may be very different.

Likewise for Scripps Mercy Hospital's Hillcrest facility versus its hospital in Chula Vista. And for some 39 other hospitals whose data are grouped with sister facilities in California, and many more across the country.
But a report released March 16 by the Leapfrog Group, which represents employers who buy health coverage, brings some sunshine to this darkness.
It shows individual rates of infection in intensive care units by individual hospital building, not in combination with other facilities in a larger system. Lower numbers are better.
"Infection rates vary significantly by hospital," said Melissa Danforth, Leapfrog's vice president for hospital ratings. "That's why Leapfrog requires hospitals to report our annual survey by location — by bricks and mortar facility — not by Medicare provider number, which may include up to seven hospitals."
Danforth said this granularity allows consumers, employers and health plans that select networks, and referring physicians, to have "location-specific information, information they can actually use to select and compare hospitals."
Case in point: On Medicare’s quality score website, Hospital Compare, UCSD's rate of catheter-associated urinary tract infections in its intensive care units is shown as 1.405, a combined rate for both hospital facilities, and one that Hospital Compare says is "worse than national benchmark." According to the Leapfrog's survey, however, Thornton Hospital's rate for these infections, known as CAUTIs, is .746, while the rate for UCSD's Hillcrest campus is much higher, 2.207.
Similarly for central-line associated bloodstream infections, or CLABSIs, on Hospital Compare UCSD's rate is listed at .936, which is "no different than a national benchmark." But in the Leapfrog survey, the scores are separated, with Thornton having .576 and Hillcrest .941.
Leapfrog segregates data for Scripps Mercy's two facilities as well. For example, Hospital Compare shows Scripps Mercy's intensive care unit CAUTI rate as .975, which is "no different than national benchmark." But in the Leapfrog survey, Scripps Mercy in Hillcrest is shown to have a rate of 1.019, while Scripps Mercy in Chula Vista has a rate of .610.
For CLABSI, the Hospital Compare rate is .524, "no different than national benchmark." But the Leapfrog survey shows .228 for Hillcrest and .322 for Chula Vista.
The Leapfrog Group’s report noted that Sharp Memorial Hospital had a CAUTI rate of 3.038, the 38th highest in the country.
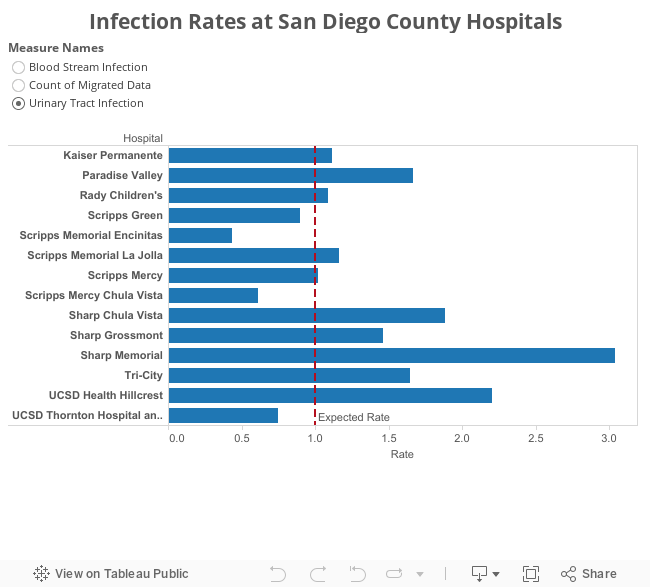
All the rates reflect a formula that compares the actual number of a hospital ICU’s infections to its “predicted” number. For example, intensive care units specializing in burn patients are compared with each other, as are units specializing in intensive care for surgical patients and or medical patients. A ratio of 1.0 means a hospital’s infection rate is the same as its expected rate.
Nationally, 56 percent of hospitals had an infection rate between 0 and 1 for CAUTI, and 92 percent had a rate between 0 and 1 for CLABSI, according to Leapfrog.
The information is important for consumers, Danforth said, not just because these infections are preventable, but they’re also expensive and deadly. “These measures really represent a hospital safety record but also give you a sense of where you may be wasting your dollars," she said.
The Leapfrog survey also gives consumers a sense of how well the hospitals have improved. For example, UCSD is said to have made "some progress" on improving its CLABSIs but has made "substantial progress" in its CAUTIs over prior reporting periods.
For CLABSIs, the Leapfrog Group considers hospitals to have met its standards if it has a rate of zero. For CAUTIs, a hospital is considered to have met its standard if it has a rate equal to or below .443.
"Hospital Compare doesn't do any true comparative performance analysis for consumers," Danforth said. Additionally, Hospital Compare reports far too many hospitals as being the same as the national average, "so it's really asking a lot for consumers to interpret the information that's on the Hospital Compare website." The Leapfrog report provides that benchmarking information.
Dr. Francesca Torriani, medical director of infection control and epidemiology for both UCSD facilities, said Leapfrog's reports showing individual hospital infection rates are important for consumers and hospital staff to know, but the measures are not perfect.
They don't account for the fact that many of the Hillcrest facility's patients are more vulnerable to infections, such as those in the ICU awaiting a liver or abdominal transplant.
"But we don't say that defensively," Torriani said. "Even though it's not for us totally adequately adjusted, we accept that's where we are, and we move on," using every analysis available to find out if any of those infections could have been prevented.
Additionally, she said, more recent rates not yet published show both hospitals have improved.
Frank Myers, UCSD's infection preventionist, and Torriani stressed that patients should not choose a hospital based on the rates of these infections. One hospital in Southern California, he said, had high infection rates, but for patients with advanced cancer, it has one of the best survival rates in the nation.
Dr. James LaBelle, chief medical officer for Scripps Health, attributed the difference to the types of patients treated in each hospital’s intensive care unit and a formula that does not adequately adjust for the severity of individual patients’ diseases.
He said it may be that patients in the ICUs at Scripps Mercy in Hillcrest are indeed sicker. “There’s a much higher acuity of patients there,” LaBelle said.
But that doesn’t diminish the importance of this facility-level data, he said. “We can compare over time how we’ve done … are we better today than we were yesterday,” he said. “Absolutely, this is useful. We track (these rates) like we track the bank account.”
He added that improvement efforts are underway for both facilities. “Nationally, we want to be in the top, not the middle of the pack, so there’s years of work to do there.”
A significant drawback in the Leapfrog survey is that it includes fewer than half of all hospitals across the country. That’s because most of the 3,812 hospitals Leapfrog surveyed declined to respond in one or both categories, including Sharp Mary Birch Hospital, Alvarado Hospital, Palomar Medical Center and Pomerado Hospital. Some of those hospitals are not eligible to report or have too few qualifying patients to reliably calculate statistics.
More than a dozen other California hospital systems with multiple facilities have data merged by Hospital Compare as well.
Hospitals report the same data to the Leapfrog survey as they do to the Centers for Disease Control and Prevention, data that Medicare uses for two programs that penalize hospitals for poor care. The Leapfrog survey uses reporting periods that cover portions of 2014 and 2015. Some of Leapfrog's data may be more up to date by three months than Hospital Compare's, Danforth said.
A CDC report in January said that although progress has been made in reducing CLABSIs, some 30,100 infections still occur in ICUs and wards of hospitals each year, increasing cost, mortality risk and prolonging hospital stays. A similar CDC report on CAUTIs says it's the fourth most common healthcare-associated infection, accounting for 13,000 deaths a year.




